

The conversation often begins after something small goes wrong.
A father misses his medicines twice in one week. A mother stops using the upstairs bedroom because climbing the stairs has become difficult. Unpaid bills begin collecting on a table. The refrigerator contains food that should have been discarded days ago.
The children see warning signs.
The parents see interference.
An adult child may begin the discussion by saying, “You need help now.” The intention is usually protection. Yet the parent may hear something very different:
“You are no longer capable of managing your own life.”
This is why conversations about elder care often become tense. The problem is not always the care option being suggested. It is how the conversation is introduced, what the parent believes will be taken away and whether the family has already made the decision without involving them.
A productive discussion should not begin with a caregiver, relocation or assisted living.
It should begin with a simpler question:
What has become difficult, and what support would help you remain independent for longer?
The parent may hear something different from what the child is saying
The child may say:
“We are worried about your safety.”
The parent may hear:
“You are becoming incapable.”
The child may say:
“We should appoint a caregiver.”
The parent may hear:
“A stranger will now control my daily routine.”
The child may say:
“This house is becoming difficult to manage.”
The parent may hear:
“You want me to leave the home I built.”
The emotional meaning of the conversation matters as much as the words.
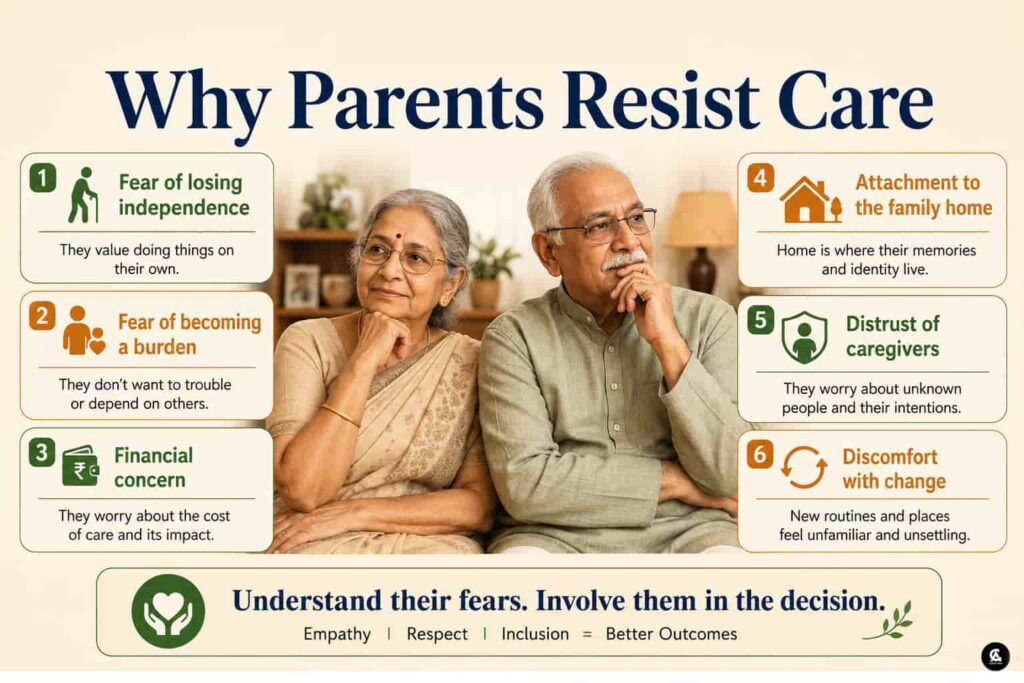
For many elderly parents, accepting care is not only about receiving assistance. It may represent:
- Loss of privacy
- Reduced authority
- Fear of dependency
- Financial insecurity
- Separation from familiar surroundings
- Concern about becoming a burden
- Anxiety about being moved against their wishes
Families should address these fears directly rather than dismissing them as stubbornness.
Do not begin the conversation with a solution
One of the most common mistakes is entering the room with a decision already made.
For example:
- “We have appointed a caregiver.”
- “You need to move closer to us.”
- “This house must be sold.”
- “We have selected an assisted-living residence.”
The parent is then invited to accept the decision rather than participate in it.
A better opening is:
“We have noticed that a few daily tasks are becoming tiring. Can we discuss what would make them easier?”
This shifts the discussion from incapability to support.
The first conversation does not need to produce the final decision. Its purpose is to understand:
- What the parent is finding difficult
- What help the parent is willing to accept
- What the family can realistically provide
- Whether the current home supports safe ageing
- What should be reviewed before the next conversation
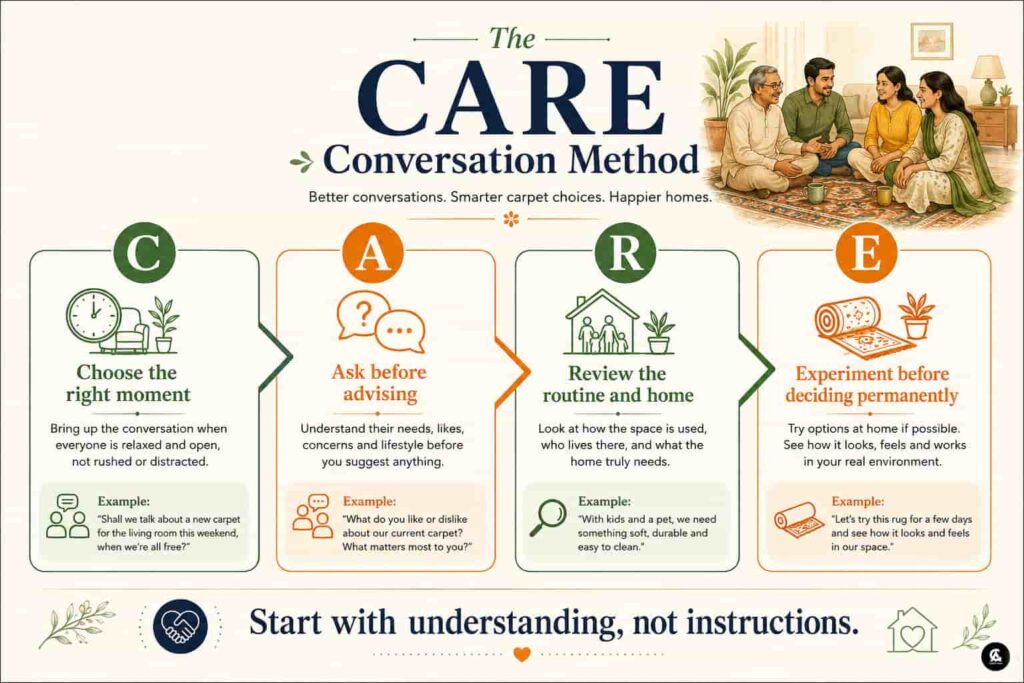
Use the CARE conversation method
A clear framework can prevent the discussion from turning into an argument.
Choose the right moment
Do not begin during:
- A family dispute
- A medical emergency
- A hospital discharge
- A financial disagreement
- A moment of embarrassment after a fall
Unless there is an immediate safety risk, select a calm time.
Allow enough time for the conversation. Do not introduce the issue while rushing to work or during a brief telephone call.
Ask before advising
Questions give parents space to describe their own experience.
Ask:
- Which daily tasks are becoming tiring?
- Do you feel comfortable using the stairs?
- Are medicines becoming difficult to manage?
- Would help with meals make the day easier?
- Is maintaining the house becoming stressful?
- What concerns you about hiring a caregiver?
- What kind of support would feel acceptable?
Parents may reveal a concern they have not previously discussed.
The family may believe that mobility is the main problem, while the parent may be more worried about loneliness, money or privacy.
Review the routine and the home together
Avoid making broad statements such as:
“You cannot live alone anymore.”
Discuss specific observations:
- The bathroom floor is slippery.
- The bedroom is located upstairs.
- Medicines are being missed.
- The lift is unreliable.
- Cooking is becoming difficult.
- The house requires frequent maintenance.
- Emergency help is not available nearby.
Specific concerns can be examined. General accusations create defensiveness.
Experiment before making a permanent decision
A trial arrangement is often easier to accept than an irreversible change.
The family can test:
- Domestic help for a few hours
- A part-time caregiver
- Weekly physiotherapy
- Meal delivery
- Bathroom modifications
- An emergency alert device
- A short stay near the children
- A trial stay in a senior-living community
After a defined period, the parent and family can review whether the arrangement improved safety and comfort.
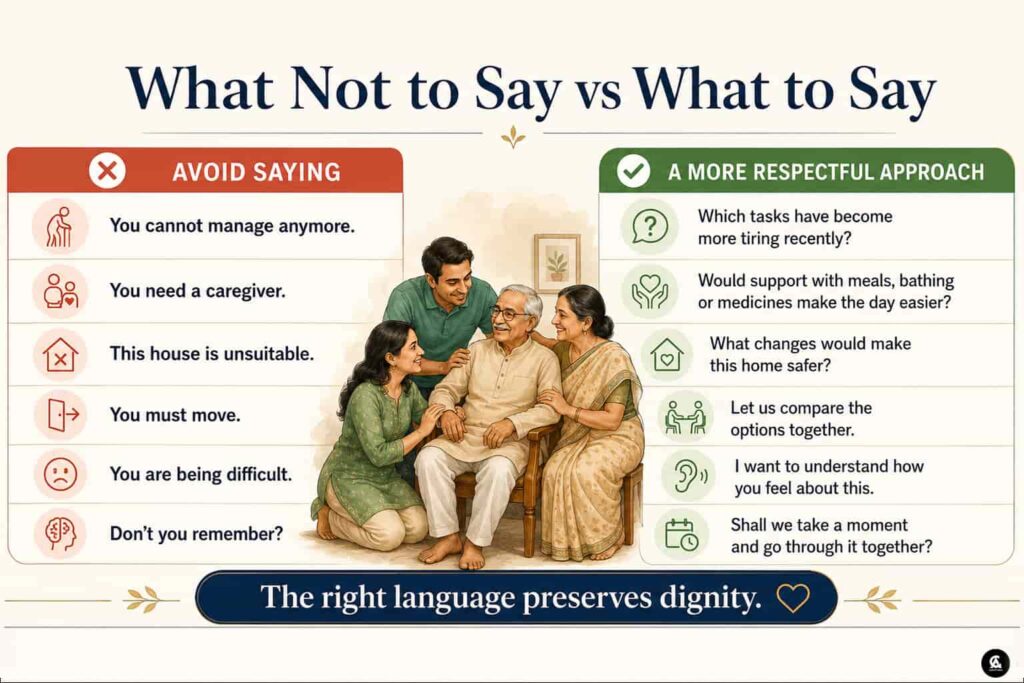
What not to say—and what to say instead
Small changes in language can completely change the direction of the discussion.
| Avoid saying | A more respectful approach |
|---|---|
| You cannot manage anymore. | Which tasks have become more tiring recently? |
| You need a caregiver. | Would support with meals, bathing or medicines make the day easier? |
| This house is unsuitable. | What changes would make this home safer and easier to use? |
| We have decided that you must move. | Let us compare the available options together. |
| You are becoming a burden. | We need a care arrangement that works comfortably for everyone. |
| You are too old to drive. | Can we review whether driving still feels safe? |
| Give me control of your bank account. | Let us create a transparent and secure system for managing payments. |
| You never listen to us. | Tell us what worries you most about accepting help. |
The objective is not to soften an already final decision.
The objective is to keep the parent involved in the decision itself.
Is the parent refusing care—or refusing to leave the home?
The family home is not merely a physical structure.
For an elderly parent, it may represent:
- A lifetime of work
- Financial security
- Memories of raising children
- Connection with a spouse
- Familiar neighbours
- Social identity
- Independence
- Routine and comfort
When children suggest relocation, parents may not only be evaluating a new apartment or residence. They may feel they are being asked to give up a part of their identity.
This is where the Carpet Area perspective becomes important.
The discussion should not begin with:
“You need to leave this house.”
It should begin with:
“Let us understand what this house needs in order to remain safe and manageable.”
The house may be creating the dependency
Not every difficulty is caused only by ageing.
The property itself may be increasing dependence.
Examples include:
- A bedroom located upstairs
- A bathroom without grab bars
- Slippery flooring
- Narrow doorways
- Poor lighting
- An unreliable lift
- No power backup
- Long distance from hospitals
- No space for a caregiver
- A large property requiring constant maintenance
- Limited social activity in the neighbourhood
A senior who struggles in a large duplex may remain more independent in a smaller, accessible apartment.
Before deciding that the parent needs more supervision, determine whether the house can be improved.
Review the home room by room
| Area | Questions the family should discuss |
| Entrance | Are steps difficult? Can a ramp or handrail be installed? |
| Bedroom | Is it on an accessible floor? Is there space for a walker? |
| Bathroom | Are grab bars, anti-skid flooring and a shower chair required? |
| Kitchen | Can meals still be prepared safely? |
| Staircase | Can the parent avoid internal stairs? |
| Building | Is the lift reliable? Is power backup available? |
| Emergency access | Can an ambulance reach the entrance quickly? |
| Location | Are hospitals, pharmacies and groceries nearby? |
| Caregiver space | Can a caregiver stay without reducing privacy? |
| Social access | Can the parent meet friends and participate in activities? |
This review should be done with the parent—not as a secret inspection conducted against them.

Different kinds of resistance require different responses
Parents may refuse care for different reasons. A single response will not work in every case.
Fear of losing independence
Offer limited support rather than complete takeover.
For example:
- Help with transportation
- Meal assistance
- Weekly check-ins
- Part-time domestic help
Show the parent that accepting help can protect independence rather than remove it.
Financial concern
Do not say:
“Do not worry about the cost.”
Instead, show the numbers.
Discuss:
- Caregiver expenses
- Home-modification costs
- Medical support
- Property maintenance
- Assisted-living fees
- What the parent can afford
- What the children can contribute
Transparency reduces suspicion.
Attachment to the family home
Do not begin with selling the property.
Consider:
- Restricting living to one floor
- Modifying the bathroom
- Hiring property-management support
- Renting a nearby accessible apartment
- Moving temporarily
- Renting the original property rather than selling immediately
Reversible options are emotionally easier to consider.
Distrust of caregivers
Allow the parent to participate in:
- Interviews
- Duty selection
- Work timings
- Background verification
- Trial periods
- Feedback and replacement decisions
A caregiver imposed without consultation may be rejected even when support is genuinely needed.
Fear of assisted living
Do not present assisted living as the final destination after failure.
Arrange:
- A guided visit
- A meal at the community
- Conversations with residents
- A short trial stay
- A written comparison of services
Parents should understand what is being proposed rather than react to stereotypes.
Denial of declining ability
Avoid saying:
“You are forgetting everything.”
Discuss observable incidents:
- Medicines were missed three times.
- The gas was left switched on.
- Two bills were unpaid.
- There were two falls in one month.
Specific events are more useful than labels.
Prepare before starting the conversation
Before approaching the parent, the family should have:
- Specific examples of concern
- A basic home-safety assessment
- Available care options
- Approximate costs
- A list of trial arrangements
- Clarity about family availability
- The parent’s known preferences
- Questions rather than instructions
The family should also decide what is genuinely urgent.
A slippery bathroom may require immediate correction. Selling the house does not.
Align siblings before speaking to the parents
Care discussions often fail because siblings enter with competing views.
One child may want a full-time caregiver. Another may want the parents to move. A third may oppose spending money. The disagreement then unfolds in front of the parents.
Before the conversation, siblings should agree on:
- What the concern actually is
- Which risks are urgent
- What can be tried first
- Available budget
- Who will coordinate care
- Who will manage medical appointments
- Who will supervise the caregiver
- Who will manage property issues
- What options will be presented
- What will not be forced immediately
Parents should not be made to choose between conflicting children.
Three realistic family situations
Situation 1: The parent refuses a caregiver
The parent says:
“I do not want a stranger in my house.”
A practical approach may be:
- Begin with domestic support rather than personal care.
- Allow the parent to interview candidates.
- Start with two or four hours daily.
- Define duties clearly.
- Review the arrangement after two weeks.
The first objective is familiarity—not complete dependence on the caregiver.
Situation 2: Parents refuse to leave a large home
The property has stairs, high maintenance and limited emergency access.
The family can:
- Conduct a home-safety review.
- Estimate modification costs.
- Move daily living to one floor.
- Appoint maintenance support.
- Test a short stay in an accessible apartment.
- Explore renting before considering a sale.
The decision should compare the emotional value of the home with the operational burden it now creates.
Situation 3: A parent needs supervision at night
The parent wanders, falls or requires medication during the night.
The family should compare:
- Separate day and night caregivers
- Nursing support
- Medical equipment
- Emergency response
- Family availability
- Assisted living
- Specialised dementia care
One live-in caregiver should not automatically be treated as uninterrupted 24-hour supervision.
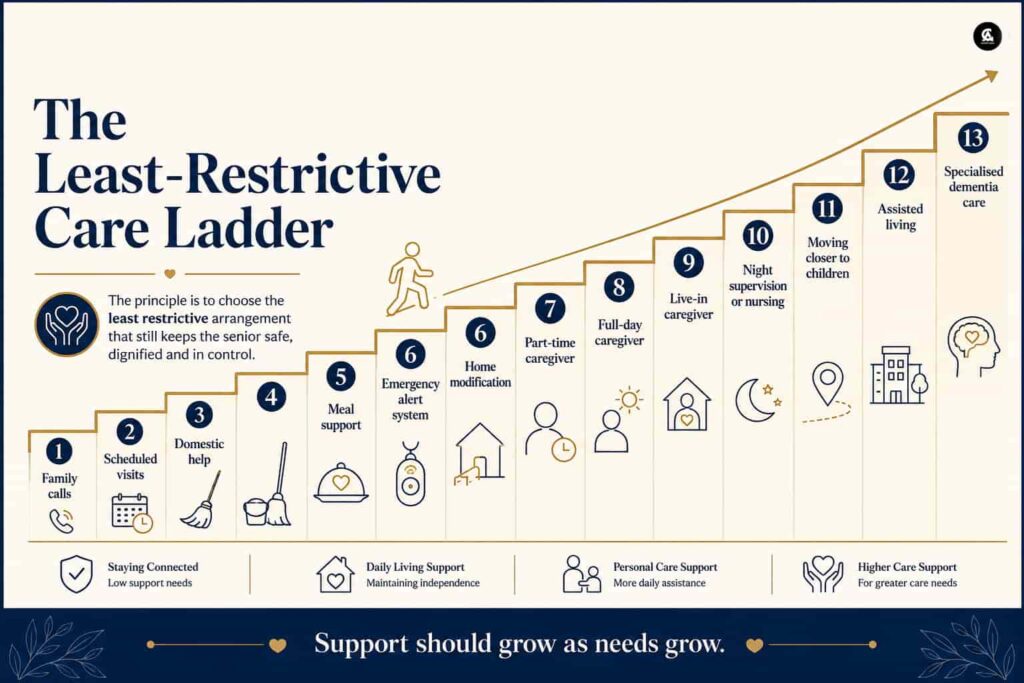
Use the least-restrictive care ladder
Families often assume there are only two choices:
- Continue exactly as before
- Move into assisted living
In reality, care can increase gradually.
A practical care ladder is:
- Regular family calls
- Scheduled visits
- Domestic help
- Meal support
- Emergency alert system
- Home modification
- Part-time caregiver
- Full-day caregiver
- Live-in caregiver
- Night supervision or nursing
- Moving closer to children
- Assisted living
- Specialised dementia care
The principle is simple:
Begin with the least restrictive arrangement that can still provide adequate safety.
However, families should not remain at a lower level merely to avoid a difficult conversation when the parent’s needs clearly require more support.
When safety can no longer wait for agreement
Respectful discussion is essential, but some situations require urgent professional involvement.
These may include:
- Repeated falls
- Wandering
- Serious medication errors
- Unsafe appliance use
- Inability to eat regularly
- Severe decline in hygiene
- Financial exploitation
- Significant confusion
- Repeated medical emergencies
- Suspected cognitive impairment
The family should not diagnose the parent.
A qualified doctor, geriatric specialist, mental-health professional, occupational therapist, legal adviser or care planner may be required depending on the concern.
Where decision-making capacity is reduced, the family may also need professional legal guidance rather than relying only on informal control of finances or property.
The first conversation should end with one practical next step
Do not try to settle every issue in one meeting.
A productive first discussion may end with:
- Scheduling a medical assessment
- Installing grab bars
- Interviewing one caregiver
- Reviewing household expenses
- Visiting one senior-living community
- Testing meal support
- Creating an emergency-contact list
- Agreeing to meet again in two weeks
A small agreed action is more valuable than a large decision that the parent resents and refuses to follow.
A final checklist for families
Before deciding on the next step, ask:
- What can the parent still manage independently?
- What has become difficult?
- What has become unsafe?
- Is the current home part of the problem?
- What support is the parent willing to try?
- What can the family provide consistently?
- Is night-time supervision required?
- Is the senior socially connected?
- Can the arrangement continue if needs increase?
- Has the parent genuinely participated in the decision?

The goal is not to win the conversation
Talking to ageing parents about care is not a negotiation in which the children must prove that they are right.
The goal is to create an arrangement that protects:
- Safety
- Independence
- Dignity
- Financial transparency
- Family relationships
- Long-term care continuity
The best care decision is not the one that gives children maximum convenience.
It is the one that remains safe and manageable while allowing the parent to retain as much choice and control as reasonably possible.
Before taking over a responsibility, ask:
Does my parent need me to make this decision—or do they only need help carrying it out?
That distinction can prevent care from becoming control.
Important note
This article provides a general family, housing and care-planning framework. It is not a substitute for medical, legal, financial or mental-capacity advice. Sudden confusion, repeated falls, major memory changes or difficulty performing daily activities should be assessed by qualified professionals.





Leave a Reply