

A family notices that its 78-year-old father has started missing medicines. He can bathe, dress and eat independently, but hospital visits are becoming difficult.
Should the family hire a caregiver?
Another family has an 82-year-old mother who needs help getting out of bed, using the bathroom and moving around the house.
Would the same caregiver arrangement work for her?
A third family is caring for a physically active parent who has dementia, wanders at night and sometimes leaves the main door open.
Can any live-in attendant safely manage that situation?
These families are all searching for “elder-care services,” but they do not need the same service.
That is where many care decisions go wrong.
A domestic helper, caregiver, nurse, physiotherapist and assisted-living residence perform different roles. Yet families often use these terms interchangeably and appoint the first available person without first assessing the senior, the house and the family’s ability to manage the arrangement.
The correct question is not:
How much does a caregiver cost?
It is:
What level of support does the senior need, and which care system can deliver it safely and consistently?
WHO’s approach to healthy ageing focuses on maintaining a person’s functional ability—not merely treating individual diseases. It also emphasises coordinated, person-centred care that supports older adults in doing what they value.
Professional elder care is not one single service
The phrase “elder care” can refer to anything from weekly help with groceries to continuous dementia supervision.
Before selecting a provider, families should understand five broad categories of support.
| Support category | Typical requirement |
|---|---|
| Household assistance | Cooking, cleaning, groceries and laundry |
| Personal care | Bathing, dressing, toileting, feeding and mobility |
| Health coordination | Medicines, appointments, reports and monitoring |
| Clinical care | Nursing procedures, wound care, catheter support or injections |
| Residential care | Accommodation, meals, personal care, activities and supervision |
Most home-based long-term care involves help with activities of daily living such as bathing, dressing, eating, taking medicines and moving safely. Residential care settings may additionally provide housing, housekeeping, meals, personal care and social activities, although services vary considerably between operators.
The service name alone is not enough. Families must examine what is actually included.
Start with function—not age
Two people aged 80 may have completely different care requirements.
One may manage:
- Personal hygiene
- Cooking
- Medicines
- Banking
- Transportation
- Social activities
Another may require assistance with:
- Bathing
- Toileting
- Eating
- Walking
- Transfers from bed to chair
- Medication
- Night-time supervision
Age tells the family very little about the actual level of support required.
A better assessment begins with the senior’s ability to perform everyday activities.
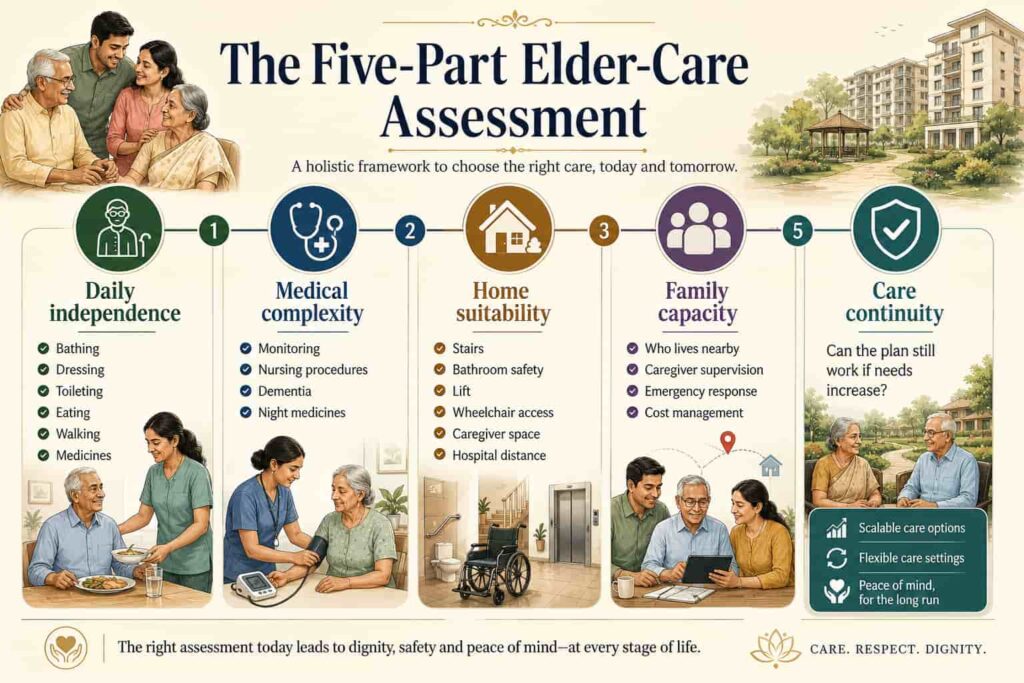
The five-part elder-care assessment
Before appointing a caregiver, nurse or residential provider, evaluate five areas.
1. Daily independence
Ask whether the senior can safely manage:
- Bathing
- Dressing
- Grooming
- Toileting
- Eating
- Getting in and out of bed
- Walking inside the house
- Using stairs
- Taking medicines
- Preparing meals
- Shopping
- Paying bills
- Attending appointments
Do not ask only whether the senior can perform a task once.
Ask whether it can be performed:
- Safely
- Regularly
- Without excessive exhaustion
- Without repeated reminders
- Without creating risk for the senior or another person
A parent may technically be able to bathe independently but may be at serious risk of slipping.
2. Medical complexity
A family must distinguish routine personal support from clinical care.
Check whether the senior needs:
- Medication reminders
- Blood-pressure checks
- Blood-sugar monitoring
- Wound dressing
- Catheter care
- Oxygen support
- Feeding assistance
- Post-operative monitoring
- Pain management
- Physiotherapy
- Dementia supervision
- Night-time medicines
- Regular nursing procedures
A caregiver may assist with daily activities, but that does not automatically make the person qualified to perform nursing duties.
The written care plan should clearly state which procedures require a licensed or appropriately trained professional.
3. Home suitability
The house is part of the care system.
Assess:
- Entrance steps
- Ramp availability
- Lift reliability
- Lift power backup
- Bathroom safety
- Bedroom location
- Wheelchair movement
- Doorway width
- Floor-level changes
- Space for a hospital bed
- Caregiver accommodation
- Ambulance access
- Distance from a hospital
- Availability of neighbours or security staff
A familiar home may provide emotional comfort while still being physically unsuitable for declining mobility.
4. Family capacity
Hiring a professional does not remove the family’s responsibilities.
Someone may still have to:
- Supervise the caregiver
- Arrange replacements
- Order medicines
- Coordinate doctors
- Make payments
- Respond to emergencies
- Resolve disputes
- Review the care plan
- Manage hospitalisation
- Maintain the property
Ask:
- Who lives nearby?
- Who can visit regularly?
- Who will respond at night?
- Who will supervise care quality?
- Who will manage expenses?
- What happens when the primary family coordinator is unavailable?
Caregiver stress is real, particularly when one family member becomes responsible for every task. The National Institute on Aging recommends planning and using practical caregiving tools rather than allowing responsibility to remain undefined.
5. Care continuity
A care arrangement should not be designed only for the senior’s present condition.
Ask what happens if the parent:
- Falls
- Is hospitalised
- Becomes wheelchair-dependent
- Develops incontinence
- Requires night supervision
- Experiences cognitive decline
- Needs nursing procedures
- Loses the current caregiver
The best arrangement is not merely the one that works today.
It is the one that can adjust without collapsing when needs increase.
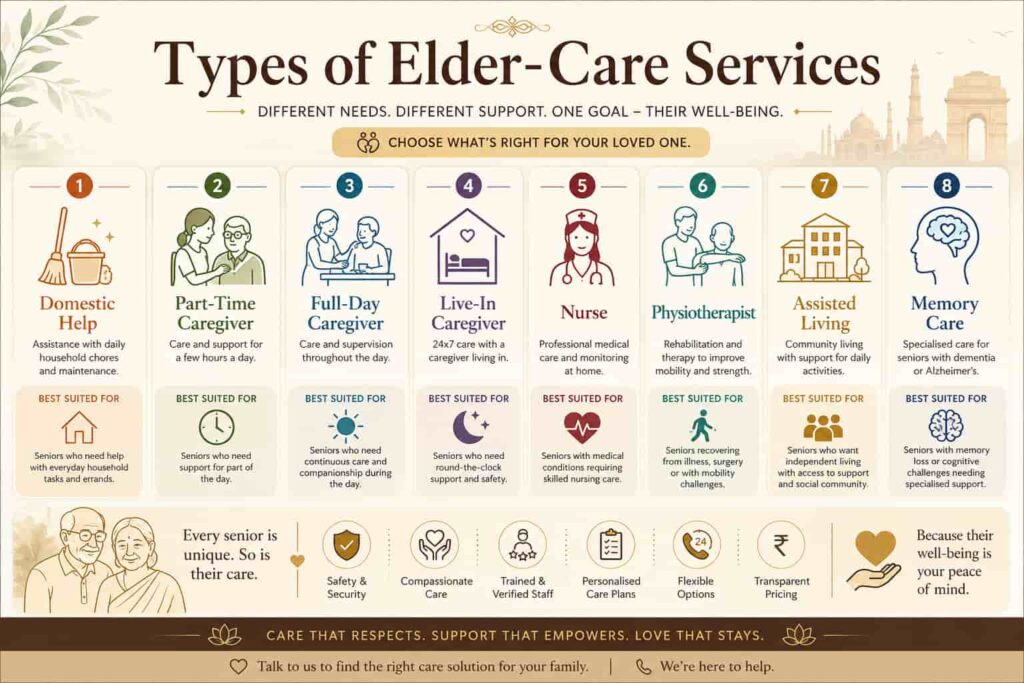
Eight elder-care options families should understand
1. Occasional family support
Suitable when the senior is largely independent but needs help with:
- Digital payments
- Appointments
- Transportation
- Documentation
- Shopping
- Property maintenance
This arrangement depends heavily on family availability and should include an emergency-contact plan.
2. Domestic help
A domestic helper may handle:
- Cooking
- Cleaning
- Laundry
- Groceries
- Basic household work
Domestic help should not be confused with personal or medical care.
A person hired for household work may not be trained to:
- Transfer a senior from bed
- Provide bathing assistance
- Handle incontinence
- Monitor health
- Support dementia behaviour
- Perform nursing procedures
3. Part-time caregiver
A part-time caregiver may help with:
- Bathing
- Dressing
- Walking
- Meals
- Companionship
- Medication reminders
- Hospital visits
This may work for a senior who remains independent for much of the day.
4. Full-day caregiver
A full-day arrangement may suit a parent who needs regular support during waking hours but does not require continuous night supervision.
The written duty list should clarify:
- Shift timings
- Personal-care responsibilities
- Meal duties
- Mobility support
- Medicine reminders
- Housekeeping expectations
- Hospital accompaniment
- Weekly leave
- Replacement arrangements
5. Live-in caregiver
A live-in caregiver provides an extended daily presence, but the term should not be mistaken for uninterrupted 24-hour alertness.
One person still requires:
- Sleep
- Breaks
- Weekly leave
- Sick leave
- Emergency replacement
Where the senior requires repeated night-time assistance, the family may need separate day and night staff.
6. Home nursing
Home nursing may be required for:
- Injections
- Wound care
- Catheter support
- Post-operative care
- Vital-sign monitoring
- Feeding support
- Clinical procedures
- Complex medication schedules
Families should confirm the professional’s qualifications, experience and exact clinical responsibilities.
7. Assisted living
Assisted living may combine:
- Accommodation
- Meals
- Housekeeping
- Personal-care assistance
- Activities
- Security
- Emergency response
- Medication support
- Community engagement
Services differ across communities. A family should never assume that a residence has 24-hour nursing, an infirmary or hospital-level care unless these are explicitly included.
8. Memory or specialised care
A physically active person with dementia may need more supervision than a mobility-limited person who is cognitively alert.
Specialised care may become necessary when there is:
- Wandering
- Severe confusion
- Unsafe appliance use
- Aggressive behaviour
- Night-time disturbance
- Repeated medication errors
- Inability to recognise risks
The environment, staffing and routines must be designed for cognitive as well as physical safety.

Use an elder-care needs score before choosing
Families can use the following practical screening tool.
Score every category:
- 0: Independent or no major concern
- 1: Some assistance required
- 2: Regular or continuous support required
| Area assessed | Score |
| Bathing and dressing | /2 |
| Toileting | /2 |
| Eating and meal support | /2 |
| Walking and transfers | /2 |
| Medication management | /2 |
| Memory and judgement | /2 |
| Night-time supervision | /2 |
| Medical or nursing procedures | /2 |
| Home accessibility | /2 |
| Family availability | /2 |
| Total | /20 |
Interpreting the score
0–5: Limited support needs
The family may consider:
- Regular check-ins
- Domestic help
- Meal support
- Emergency alert system
- Part-time assistance
6–11: Regular support required
Consider:
- Part-time or full-day caregiver
- Home modification
- Physiotherapy
- Structured medication support
- Regular family supervision
12–16: High care requirement
Evaluate:
- Full-time or live-in caregivers
- Separate night support
- Nursing
- Assisted living
- Greater medical coordination
17–20: Structured or specialised care
A comprehensive professional assessment may be required, particularly if there is dementia, major medical complexity or dependence across most daily activities.
This score is a family screening tool. It is not a medical diagnosis or substitute for professional assessment.
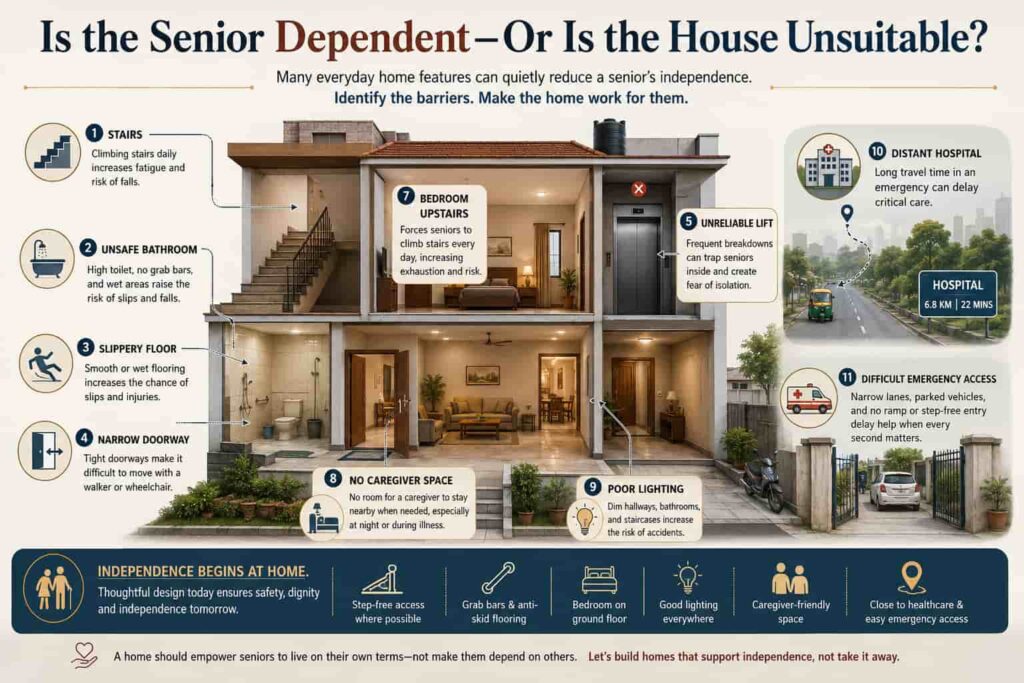
Is the senior dependent—or is the house unsuitable?
Families often respond to mobility decline by hiring more staff.
Sometimes the property should be examined first.
Consider the following situations:
- The parent needs help bathing because the bathroom is slippery.
- The parent cannot access the bedroom without climbing stairs.
- The senior depends on others because the building lift frequently fails.
- The wheelchair cannot pass through narrow doorways.
- The caregiver has nowhere suitable to sleep.
- An ambulance cannot approach the building entrance.
- The nearest hospital is too far away for urgent care.
In such cases, the house may be increasing the senior’s dependence.
Healthy ageing is partly about creating environments that allow people to continue doing what they value. A person does not need to be completely free of disease to retain meaningful independence when health conditions and the environment are managed well.
Conduct a home-care readiness audit
Entrance
Check:
- Step-free access
- Ramp slope
- Handrails
- Lighting
- Wheelchair clearance
- Ambulance approach
- Security response
Bedroom
Check:
- Accessible floor
- Bathroom proximity
- Bed height
- Walker space
- Emergency alert
- Caregiver access
- Medical-equipment space
Bathroom
Check:
- Grab bars
- Anti-skid flooring
- Shower chair
- Raised toilet seat
- Wide doorway
- Easy-to-use fixtures
- Assisted-bathing space
Building
Check:
- Lift reliability
- Power backup
- Fire safety
- Security
- Wheelchair-friendly common areas
- Emergency exit access
Location
Check:
- Hospital distance
- Pharmacy access
- Grocery delivery
- Family proximity
- Social activity
- Public transport
- Ambulance availability
Improving these areas may preserve independence and reduce the amount of hands-on assistance required.
Three families, three different care solutions
Family 1: Independent mother living alone
She manages personal hygiene and meals but needs help with digital payments, appointments and transportation.
A practical plan may include:
- Weekly family coordination
- Domestic help
- Emergency alert
- Medicine organiser
- Part-time companionship
- Social activities
Moving her into residential care immediately may be unnecessary.
Family 2: Partially dependent father in an inaccessible house
He needs bathing assistance and uses a walker. His bedroom is upstairs, and the bathroom lacks grab bars.
A practical plan may include:
- Ground-floor bedroom
- Bathroom modification
- Full-day caregiver
- Physiotherapy
- Accessible transportation
- Regular care review
The family should first determine whether the home can be modified safely and economically.
Family 3: Parent with dementia and night wandering
The parent walks independently but forgets medicines, becomes confused and attempts to leave the house at night.
A practical plan may require:
- Continuous supervision
- Secure doors and exits
- Structured routine
- Separate night staffing
- Trained dementia caregiver
- Memory-care assessment
Physical strength should not be mistaken for safe independence.

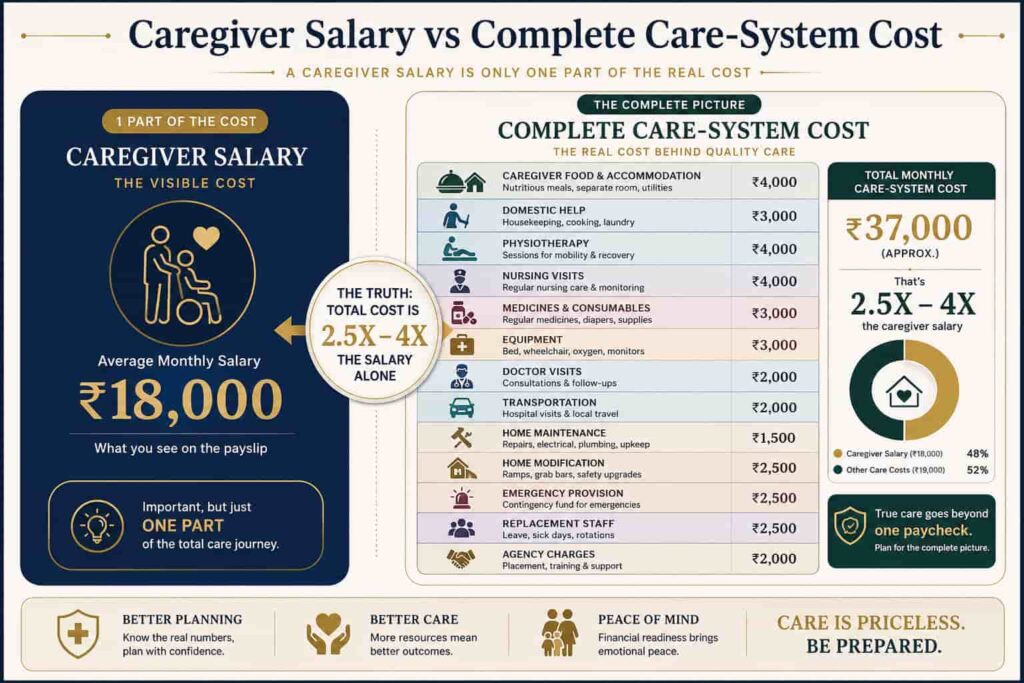
The caregiver’s salary is not the complete home-care cost
Suppose a family hires a live-in caregiver for ₹30,000 per month.
The complete home-care budget may also include:
- Caregiver food and accommodation
- Domestic help
- Physiotherapy
- Nursing visits
- Medicines and consumables
- Medical equipment
- Doctor visits
- Transportation
- Property maintenance
- Home modification
- Emergency provision
- Replacement staff
- Agency charges
A residential-care fee may appear higher because it could include housing, meals, housekeeping, security, activities and some care services.
The two amounts should not be compared until the family creates a like-for-like service list.
Build the complete cost sheet
| Cost category | Home arrangement | Residential arrangement |
| Accommodation | Existing home cost | Included or separately charged |
| Caregiver | Separate salary | May be included by care level |
| Meals | Family arrangement | Commonly included |
| Housekeeping | Separate | Commonly included |
| Utilities | Family responsibility | May be included |
| Nursing | Additional | Varies by provider |
| Activities | Separately arranged | Commonly available |
| Emergency response | Must be arranged | Usually structured |
| Staff replacement | Family or agency | Operator responsibility |
| Maintenance | Family responsibility | Usually operator-managed |
The family should obtain a written quotation rather than relying on a headline monthly price.
A caregiver, nurse and domestic helper are different roles
Expecting one person to perform every task may create unsafe care and frequent conflict.
A written duty matrix can prevent confusion.
| Responsibility | Domestic help | Caregiver | Nurse |
| Cleaning and laundry | Primary | Limited | No |
| Cooking | Possible | If agreed | No |
| Bathing assistance | No or limited | Yes | If clinically needed |
| Mobility support | No or limited | Yes | Yes when medically relevant |
| Medication reminders | No | Yes | Yes |
| Giving injections | No | No unless qualified | Yes |
| Wound care | No | No unless qualified | Yes |
| Vital monitoring | No | Basic if trained | Clinical |
| Companionship | Limited | Yes | Limited |
| Dementia supervision | No | Specialist caregiver | Clinical support |
Actual duties depend on training, qualifications and the written service contract.
Verify the provider before allowing access to the home
A caregiver may gain access to:
- Medicines
- House keys
- Personal documents
- Financial information
- Daily routines
- Jewellery and valuables
- Medical history
Families should verify more than personality and availability.
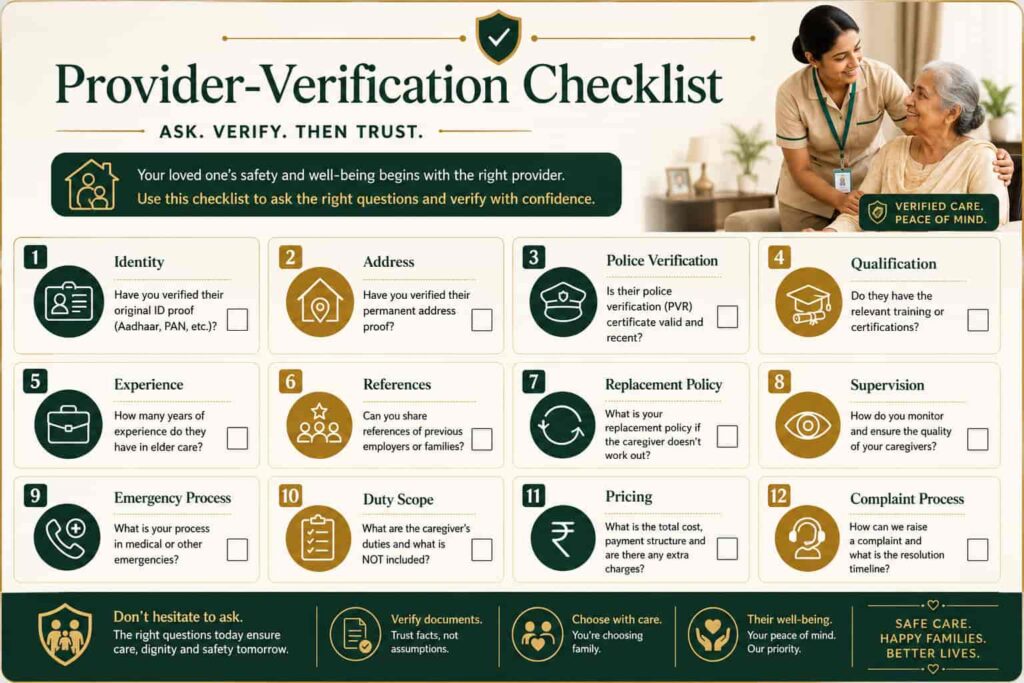
Provider-verification checklist
| Verification area | Questions to ask |
| Identity | Are government-issued documents verified? |
| Address | Is the permanent address recorded? |
| Police verification | Has background verification been completed? |
| Qualification | What tasks is the caregiver trained to perform? |
| Experience | Has the person handled similar care needs? |
| References | Can previous employers be contacted? |
| Replacement policy | What happens during leave or resignation? |
| Supervision | Does the agency monitor staff performance? |
| Emergency process | Who responds during a crisis? |
| Duty scope | Are responsibilities written clearly? |
| Pricing | What is included and excluded? |
| Complaint process | How are concerns escalated? |
Do not rely only on verbal promises.
Questions to ask an assisted-living provider
Ask for written clarity on:
- Staff-to-resident availability
- Day and night coverage
- Nursing hours
- Medicine management
- Doctor visits
- Emergency-response process
- Hospital tie-ups
- Meals and dietary support
- Housekeeping
- Activities
- Dementia support
- Additional-care charges
- Refund and exit terms
- Trial-stay availability
Residential facilities may provide very different combinations of housing, personal care, meals, social activities and medical support. Families should compare actual service inclusions rather than labels.
When home care may be enough
Home care may remain suitable when:
- The senior is largely independent
- Medical requirements are limited
- The home is accessible
- Family members live nearby
- Night supervision is unnecessary
- Reliable caregivers are available
- Replacements can be managed
- Social isolation is not severe
Home care offers the advantage of familiar surroundings, routines and neighbourhood relationships.
However, familiarity should not be used to justify an unsafe or unreliable arrangement.
When assisted living deserves consideration
Assisted living may offer better continuity when:
- The parent lives alone
- Children live far away
- Caregivers change repeatedly
- Meal and household management are deteriorating
- Falls or medication mistakes are increasing
- The home cannot be modified adequately
- The senior needs regular activities and companionship
- Family coordination has become unsustainable
- Daily support and emergency response must work together
The decision should be based on the senior’s needs, preferences, functional ability, financial resources and available housing options.
When specialised care may be necessary
Professional medical or specialised-care assessment may be required when there is:
- Dementia with wandering
- Significant cognitive decline
- Feeding support
- Catheter care
- Complex wound management
- Regular injections
- Repeated night emergencies
- Severe mobility dependence
- Palliative-care requirements
- Need for continuous clinical monitoring
Families should not expect a general caregiver to manage complex clinical needs without appropriate training and supervision.
Use the CARE-SYSTEM decision framework
Before making the final decision, ask seven questions.
C — Capability
What can the senior still manage independently?
A — Assistance
Which daily activities require regular help?
R — Risk
Are there falls, wandering, medication mistakes or emergency concerns?
E — Environment
Can the current home safely support reduced mobility and future care?
S — Supervision
Is day, night or continuous supervision required?
Y — Year-ahead needs
Can this care arrangement adapt if dependency increases?
S — Sustainability
Can the family manage the cost, staffing and coordination for the long term?
A care decision should not be based on one emotional conversation or one provider’s sales presentation.
The right care arrangement protects function, dignity and continuity
Professional elder care should not remove the family from the process.
It should create a stronger structure around the senior.
The family’s role may shift from performing every task personally to:
- Selecting the right service
- Monitoring care quality
- Protecting the senior’s preferences
- Managing finances transparently
- Maintaining emotional involvement
- Reviewing the care plan
India’s older population is expected to grow substantially over the coming decades, increasing the importance of housing, care and support systems that can respond to different levels of independence and dependency.
The best solution is not necessarily the cheapest service or the most premium residence.
It is the arrangement that answers four questions honestly:
- Can the senior remain safe?
- Can the senior retain meaningful independence?
- Can the family manage the arrangement consistently?
- Can the care system continue when needs increase?
That is the difference between hiring help and building a care plan.

Important note
This article provides a general family, housing and elder-care planning framework. It does not diagnose medical conditions or prescribe a specific care arrangement. Families should seek qualified medical, nursing, legal and financial advice where the senior has complex needs, cognitive impairment or reduced decision-making capacity.
Sources:-
- WHO — Integrated Care for Older People (ICOPE)
- WHO — Healthy Ageing and Functional Ability
- WHO — Ageing and Health
- UNFPA — India Ageing Report 2023 PDF
- UNFPA — Key Findings from the India Ageing Report 2023





Leave a Reply