
It is 2:30 in the morning.
Your father wakes to use the bathroom. He sits at the edge of the bed, searches for his slippers and walks through a dimly lit passage. The bathroom is several metres away, a loose rug lies near the door, and the light switch is difficult to reach.
The family may describe the problem as “poor sleep after 60.”
But the real concern may be larger.
Why did he wake up? Was it pain, medication, frequent urination, anxiety, breathing difficulty or a change in his natural sleep cycle? And once he woke up, was the house designed to help him move safely?
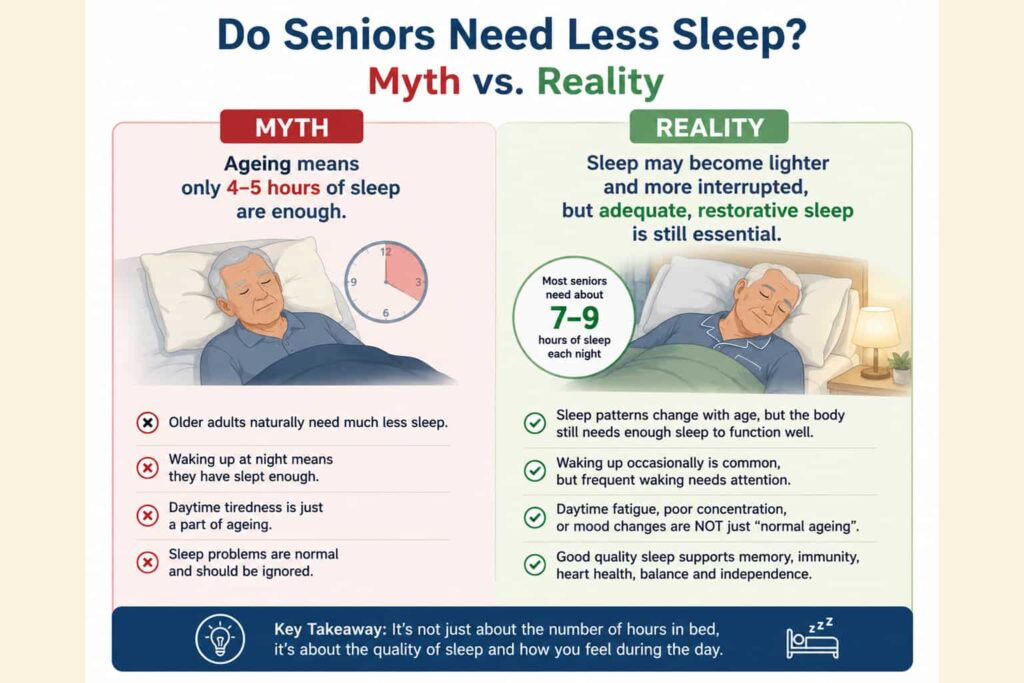
Sleep commonly becomes lighter and more fragmented with age. Older adults may wake more frequently and earlier than they did when they were younger. However, they do not automatically stop needing adequate sleep. The National Institute on Aging says older adults generally need around seven to nine hours of sleep each night.
Therefore, poor sleep should not simply be dismissed as “part of old age.”
The right approach is to examine four areas together:
- The senior’s natural sleep pattern
- Health conditions and medication
- Daytime routine and emotional well-being
- The bedroom and wider home environment
Older adults do not automatically need much less sleep
One of the most common misconceptions is that seniors require only four or five hours of sleep.
Ageing may change the way sleep is experienced. A senior may:
- Become sleepy earlier in the evening
- Wake earlier in the morning
- Take longer to fall asleep
- Wake several times during the night
- Spend less time in deep sleep
- Become more aware of being awake
MedlinePlus notes that older adults tend to wake more often and spend less time in deep sleep. Their total sleep may decrease slightly, but lighter and interrupted sleep can make them feel as though they slept much less than they actually did.
The important question is not only:
How many hours was the senior in bed?
It is:
Was the sleep restorative, and could the senior function safely and comfortably the next day?
Persistent daytime exhaustion, confusion, irritability or difficulty concentrating deserves attention even when the senior appears to spend enough time in bed.
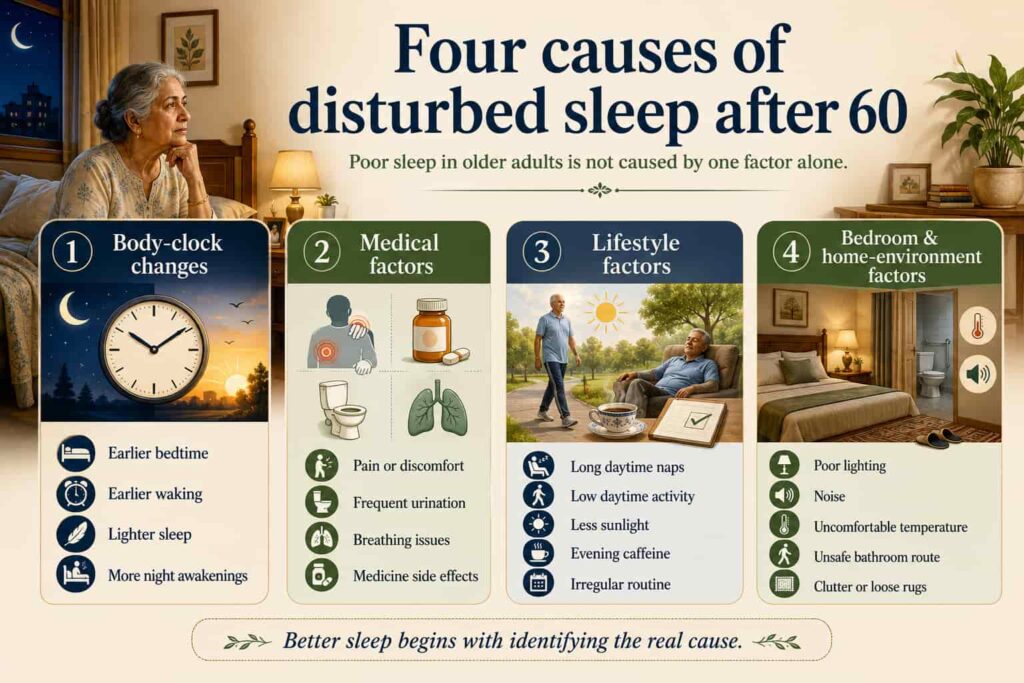
The four causes of disturbed sleep after 60
Poor sleep rarely has one single cause. Families should review four connected areas before searching for a quick solution.
1. Natural sleep-pattern changes
The body’s internal clock may shift with age. This can make a senior feel tired earlier and wake earlier.
Sleep may also become lighter, which means ordinary sounds, discomfort or the need to use the bathroom can cause more frequent awakening.
An earlier bedtime is not automatically a problem if the senior:
- Receives adequate sleep
- Feels refreshed in the morning
- Remains active during the day
- Does not experience severe sleepiness
- Can safely manage daily activities
2. Health and medication factors
Sleep may be interrupted by:
- Arthritis or chronic pain
- Breathing difficulty
- Frequent night-time urination
- Heart-related symptoms
- Diabetes-related discomfort
- Anxiety or depression
- Restless legs
- Medication side effects
Some medicines can cause daytime drowsiness, difficulty sleeping, dizziness or increased night-time urination. Prescribed medicines should never be stopped, rescheduled or altered without consulting a doctor or pharmacist.
Families should prepare a complete list of medicines, including over-the-counter products and sleep supplements, before seeking medical advice.
3. Lifestyle and emotional factors
A senior may remain awake at night because the body has not received enough daytime activity, natural light or social stimulation.
Possible contributors include:
- Long afternoon naps
- Limited physical activity
- Very little morning sunlight
- Evening caffeine
- Irregular sleeping times
- Loneliness
- Bereavement
- Anxiety
- Excessive screen use before bed
A regular sleep schedule, suitable daytime exercise and limiting late naps can support healthier sleep. The type and intensity of activity should match the senior’s health and mobility.
4. Bedroom and home-environment factors
A room may look comfortable during the day but become unsafe and disruptive at night.
Sleep may be affected by:
- Traffic or lift noise
- Excessive outdoor light
- Poor ventilation
- Uncomfortable room temperature
- A difficult bed height
- An inaccessible bathroom
- Fear of falling
- Cluttered walking space
- Loose rugs or wires
- No light within reach
- Lack of emergency support
This is where a general sleep article becomes a Carpet Area issue.
The physical home can either protect independence or increase dependence.
Is the bedroom disturbing the sleep?
Before buying a new mattress, sleep supplement or expensive device, inspect the complete bedroom.
A senior-friendly bedroom should help the person:
- Enter and leave the bed safely
- Reach the bathroom without obstacles
- Control lighting easily
- Access a phone or emergency alert
- Use a walker where required
- Maintain a comfortable temperature
- Rest without excessive noise
- Receive help quickly during an emergency
The design should support both sleep quality and night-time movement.
Bedroom location matters
A first-floor bedroom may have worked perfectly for 20 years. It may become unsuitable when the senior develops:
- Knee pain
- Reduced balance
- Breathlessness
- Urinary urgency
- Weakness after hospitalisation
- Fear of stairs
Where possible, the bedroom should be:
- On an accessible floor
- Close to a bathroom
- Away from unnecessary household noise
- Within easy reach of family or caregiver support
- Connected to a clear emergency exit route
Moving the bedroom to the ground floor may preserve independence without requiring the senior to leave the home.
The route to the bathroom is part of the sleep environment
Many seniors wake during the night to use the bathroom.
At that moment, they may be:
- Sleepy
- Disoriented
- Without spectacles
- In a hurry
- Feeling dizzy
- Under the effect of medication
The route should be checked for:
- Loose rugs
- Electrical wires
- Low furniture
- Slippery flooring
- Poor lighting
- Sudden level changes
- Unstable hand support
- Doors that are difficult to open
The CDC’s home fall-prevention checklist recommends keeping the path between the bed and bathroom clear, placing an easy-to-reach light near the bed and using a nightlight along a dark route. It also recommends non-slip bathroom surfaces and grab bars where support is needed.

Bed height can affect night-time safety
A visually impressive bed is not necessarily senior-friendly.
The senior should ideally be able to:
- Sit comfortably at the edge
- Place both feet firmly on the floor
- Stand without excessive effort
- Reach a walker or support device
- Return to bed without climbing or dropping down
A bed that is too low can make standing difficult. A bed that is too high may increase instability.
There should also be enough space around the bed for:
- Safe movement
- A walking aid
- A caregiver, if required
- Medical equipment
- Emergency access
Lighting must support sleep and movement
The bedroom needs two kinds of lighting.
Sleep-supportive lighting
- Warm and low-intensity bedside light
- Curtains that control outside light
- Reduced screen glare
- No bright overhead light immediately before sleep
Safety lighting
- A switch within reach of the bed
- Low-level night lighting
- Motion-sensor lighting where appropriate
- A clearly lit route to the bathroom
- Reliable backup lighting during power cuts
The aim is not to keep the bedroom bright throughout the night. It is to prevent complete darkness from turning an ordinary bathroom visit into a fall risk.
Noise, temperature and ventilation matter
Sleep may be disturbed by:
- Traffic
- Lift machinery
- Generator noise
- Television in a nearby room
- Household activity
- Construction
- Street lighting
- Direct cold air from an air conditioner
- Excessive heat or humidity
Families choosing or modifying a senior’s bedroom should assess the room at night—not only during a daytime property visit.
A bedroom facing a busy road may seem acceptable at 11 a.m. but become unsuitable for a light sleeper after 10 p.m.
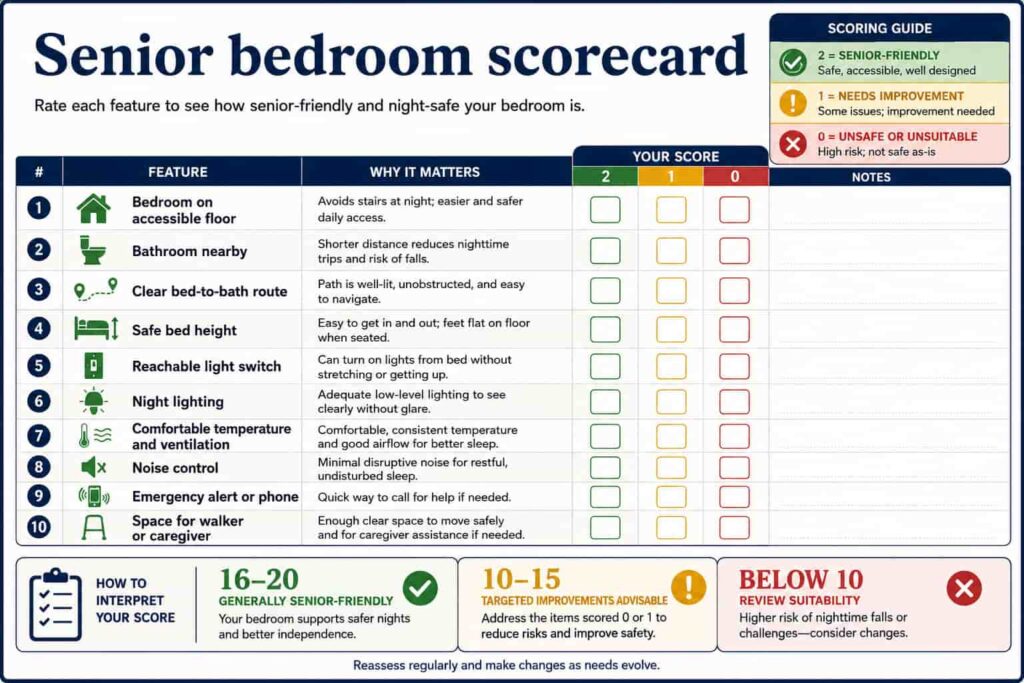
The senior sleep-friendly bedroom score
Use the following tool to assess the room.
Score each feature:
- 0: Unsafe or unsuitable
- 1: Usable but needs improvement
- 2: Senior-friendly
| Bedroom feature | Score |
|---|---|
| Bedroom is on an accessible floor | /2 |
| Bathroom is nearby | /2 |
| Bed-to-bathroom route is clear | /2 |
| Bed height is safe | /2 |
| Light switch is within reach | /2 |
| Night lighting is available | /2 |
| Temperature and ventilation are comfortable | /2 |
| Noise is reasonably controlled | /2 |
| Emergency alert or telephone is accessible | /2 |
| Space is available for a walker or caregiver | /2 |
| Total | /20 |
16–20: The bedroom is generally senior-friendly.
10–15: Targeted improvements are advisable.
Below 10: The room’s long-term suitability should be reviewed.
This is a practical screening tool, not a medical or architectural certification.

A night-time fall is not only a health issue
More than one in four people aged 65 and above falls each year, according to the CDC. Home hazards such as clutter, uneven steps and loose rugs can contribute to the risk.
A senior waking at night may face several risks at the same time:
- Reduced alertness
- Poor vision
- Urgent bathroom need
- Balance difficulty
- Sedating medicine
- Slippery flooring
- No support nearby
This is why sleep planning and fall prevention should not be treated as separate subjects.
The family should ask:
If the senior wakes three times tonight, can every journey from the bed to the bathroom happen safely?
Four family situations that require different responses
Situation 1: The senior repeatedly wakes to use the bathroom
Possible contributors include:
- Frequent urination
- Medicine timing
- Diabetes or another medical issue
- Bathroom located too far away
- Difficult bed exit
- Fear of falling
The family can:
- Improve the walking route
- Install appropriate night lighting
- Review bathroom safety
- Keep support devices within reach
- Discuss persistent night-time urination with a doctor
Changing the route does not replace medical assessment. Both may be necessary.
Situation 2: The senior sleeps during the day and remains awake at night
Possible contributors include:
- Long naps
- Limited daytime activity
- Low sunlight exposure
- Loneliness
- Medicine-related drowsiness
- Lack of routine
The first response should not be sleeping medication.
The family can begin with:
- A consistent waking time
- Suitable morning activity
- Natural daylight
- Shorter or earlier naps
- Social engagement
- Professional medication review
Situation 3: The senior snores loudly and remains exhausted
Loud snoring alone does not confirm a disorder. However, snoring combined with gasping, choking, breathing interruptions or severe daytime sleepiness can indicate possible sleep apnea and should be discussed with a healthcare provider. Sleep apnea causes breathing to stop and restart repeatedly and can prevent the person from receiving adequate oxygen and restorative sleep.
A quieter room or better mattress cannot correct a breathing disorder.
Situation 4: The senior fears getting out of bed at night
The fear may follow:
- A previous fall
- Dizziness
- A dark bathroom route
- Unstable furniture
- An inaccessible switch
- Bedroom stairs
- Lack of emergency support
The family should not simply tell the parent to “be careful.”
The environment should be changed so that safety does not depend entirely on caution.
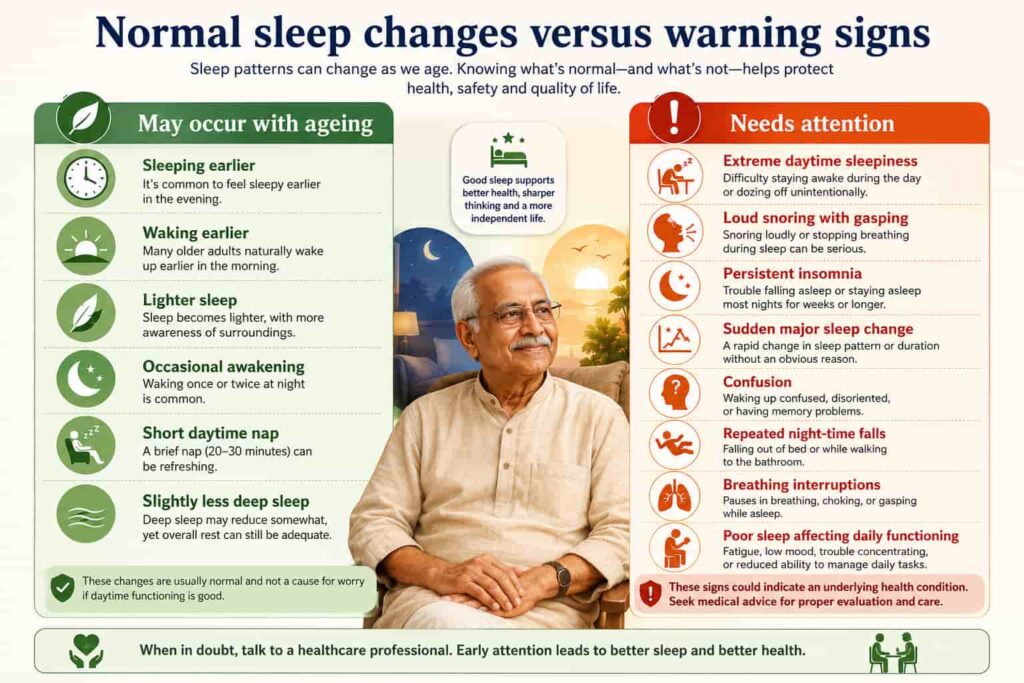
Normal age-related change versus a warning sign
| May occur with ageing | Deserves further attention |
| Becoming sleepy somewhat earlier | Extreme daytime sleepiness |
| Waking somewhat earlier | Loud snoring with gasping or choking |
| Lighter sleep | Persistent difficulty sleeping |
| Occasional night awakening | Sudden major change in sleep behaviour |
| Short daytime nap | Repeated confusion or memory difficulty |
| Slight reduction in deep sleep | Falls or near-falls during the night |
| Taking longer to settle occasionally | Breathing that repeatedly stops and restarts |
| Feeling awake briefly at night | Poor sleep affecting daily functioning |
Persistent sleep difficulty can be associated with depression, medical conditions and sleep disorders. Severe daytime sleepiness, repeated breathing interruptions or substantial changes in functioning should not be accepted as inevitable ageing.
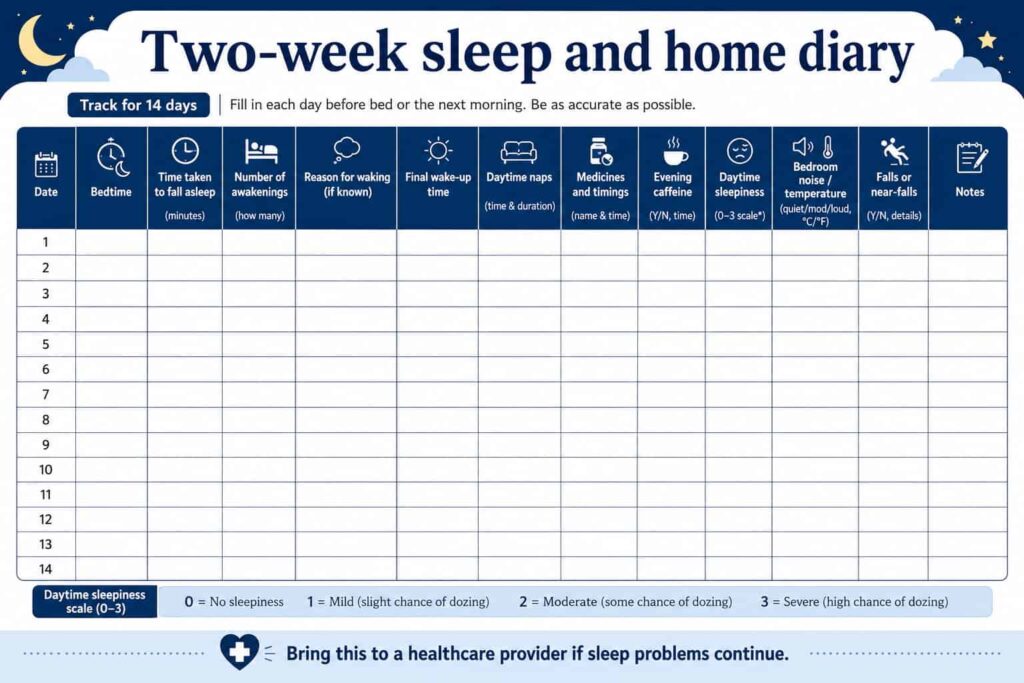
Keep a two-week sleep and home diary
Families often visit a doctor with a broad statement:
“My mother does not sleep properly.”
A sleep diary provides more useful information.
Record the following for 14 days:
| Information to record | Why it helps |
| Time the senior went to bed | Shows the sleeping routine |
| Approximate time taken to sleep | Identifies difficulty falling asleep |
| Number of awakenings | Shows sleep fragmentation |
| Reason for waking | Pain, bathroom, noise, anxiety or breathing |
| Final wake-up time | Shows the full pattern |
| Daytime naps | Identifies possible daytime interference |
| Medicines and timings | Supports medication review |
| Evening caffeine | Identifies possible stimulation |
| Daytime sleepiness | Shows functional effect |
| Falls or near-falls | Identifies environmental risk |
| Bedroom temperature or noise | Connects sleep with the room |
The NHLBI recommends using a sleep diary to track sleep quality, sleep duration, medicine use, caffeine and daytime sleepiness, and bringing the information to a healthcare provider.
Do not start sleeping medicines without medical advice
Older adults may respond differently to medicines, and some sleep medicines can contribute to confusion, dependence, delirium or falls when used inappropriately or for prolonged periods.
Before speaking to a healthcare provider, prepare:
- A list of prescribed medicines
- Over-the-counter products
- Supplements
- Medicine timings
- Recent dosage changes
- Dizziness or imbalance
- Daytime drowsiness
- Night-time urination
- Recent falls
- Caffeine and alcohol use
Do not stop or alter a prescribed treatment independently.
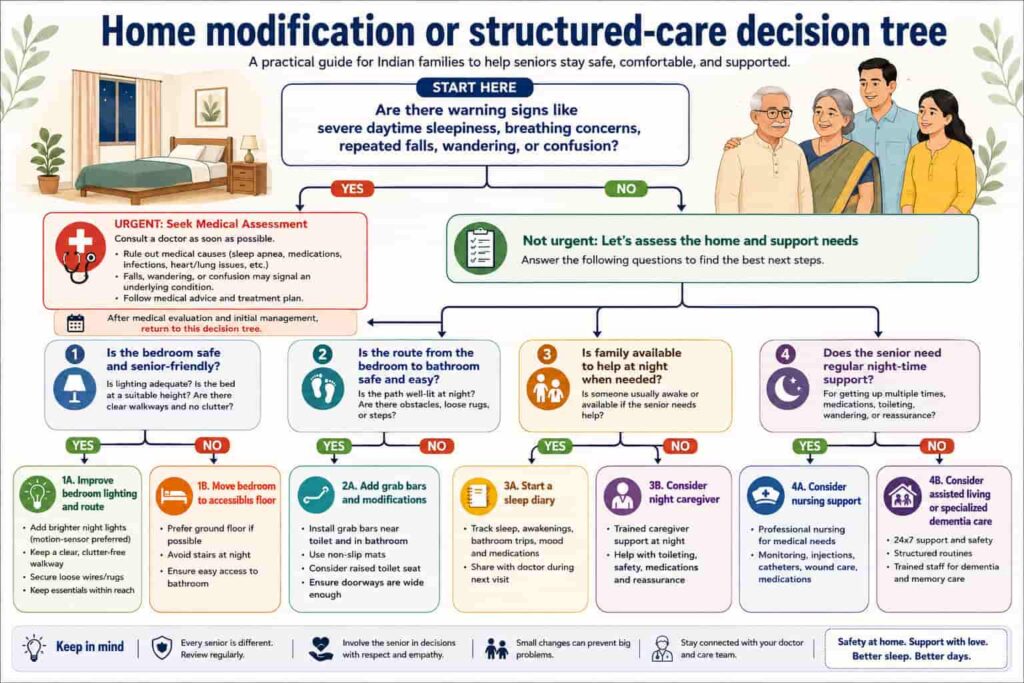
When home modification may be enough
Home improvement may solve much of the practical problem when:
- The senior is mostly independent
- The main concern is bathroom access
- The walking route can be cleared
- Lighting can be improved
- The bedroom can be moved to an accessible floor
- Family support is nearby
- No continuous medical monitoring is needed
- Night waking is limited and manageable
Possible modifications include:
- Moving the bedroom
- Installing bedside and pathway lighting
- Removing loose rugs
- Adding grab bars
- Improving bathroom flooring
- Adjusting furniture
- Providing an emergency alert
- Creating space for a walker
When the concern is larger than the bedroom
Professional or structured care deserves consideration when:
- The senior wanders at night
- Dementia causes confusion
- Falls continue despite modification
- Medication is required during the night
- Breathing concerns are present
- The senior needs assistance every time they stand
- One caregiver cannot provide reliable night coverage
- Family members live far away
- The property cannot be modified adequately
- Night-time care has become unsustainable
In these situations, the family may need to compare:
- Night caregiver support
- Qualified nursing
- Home care with multiple shifts
- Moving the parent closer
- Assisted living
- Specialised dementia care
The decision should compare complete care systems—not only the emotional preference to remain at home.
A practical family action plan
Do not try to solve every sleep concern in one night.
Start with these steps:
- Ask the senior how the sleep feels—not only how long it lasts.
- Keep a two-week sleep diary.
- List medicines and their timings.
- Inspect the bedroom after dark.
- Walk the exact route to the bathroom.
- Remove rugs, wires and unstable furniture.
- Check the bed height and lighting.
- Improve daytime activity and routine where suitable.
- Seek medical advice for persistent or serious symptoms.
- Review whether the existing home can support future needs.
The bedroom should protect both rest and independence
A senior-friendly bedroom is not merely a room with a large bed and attractive décor.
It should help the person:
- Sleep comfortably
- Wake safely
- Reach the bathroom
- Call for help
- Maintain privacy
- Continue living with confidence
Poor sleep after 60 may involve ageing, health, medication, routine and emotional well-being.
But the home also matters.
Before accepting sleeplessness, repeated night-time waking or fear of movement as inevitable, examine the complete situation.
Ask:
Is the senior unable to sleep—or is the bedroom making sleep and night-time movement unnecessarily difficult?
Sometimes the most valuable intervention is medical.
Sometimes it is behavioural.
And sometimes it begins by moving a light switch, removing a loose rug or choosing a safer bedroom.
Important note
This article is for general education and home-planning awareness. It does not diagnose or treat sleep disorders. Persistent insomnia, gasping, breathing interruptions, severe daytime sleepiness, repeated falls, sudden confusion or major changes in behaviour should be assessed by qualified healthcare professionals.
Sources:-
- National Institute on Aging: Sleep and Older Adults
- MedlinePlus: Aging Changes in Sleep
- National Heart, Lung, and Blood Institute: Sleep Apnea and Sleep Diary
- CDC STEADI: Older-Adult Home Fall-Prevention Guidance
- Jeevin Senior Care: Sleep Changes After 60





Leave a Reply